Printable Hippa Form
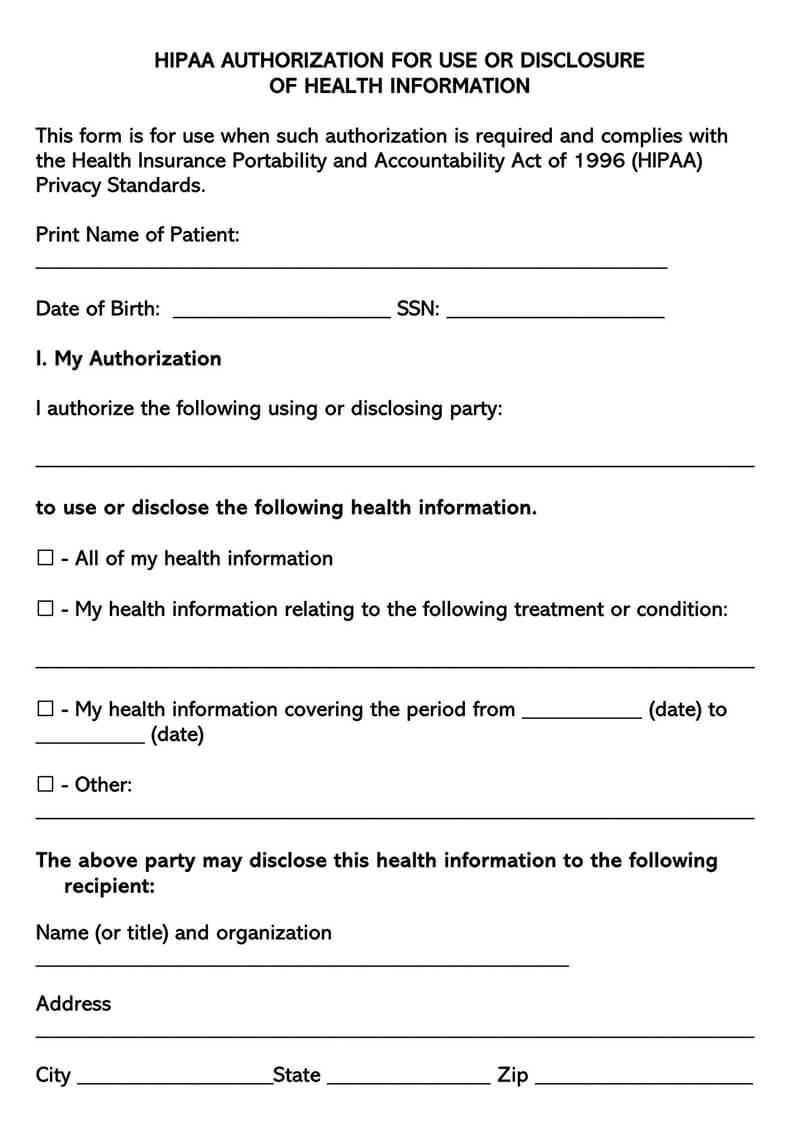
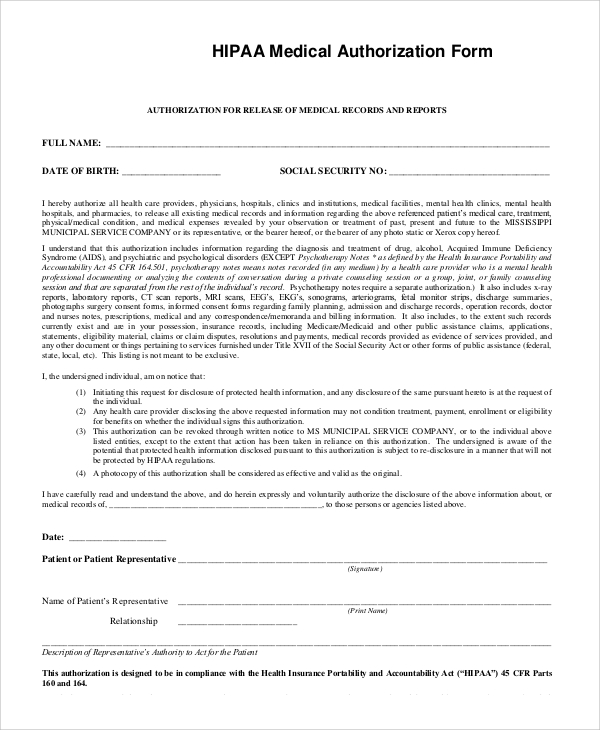
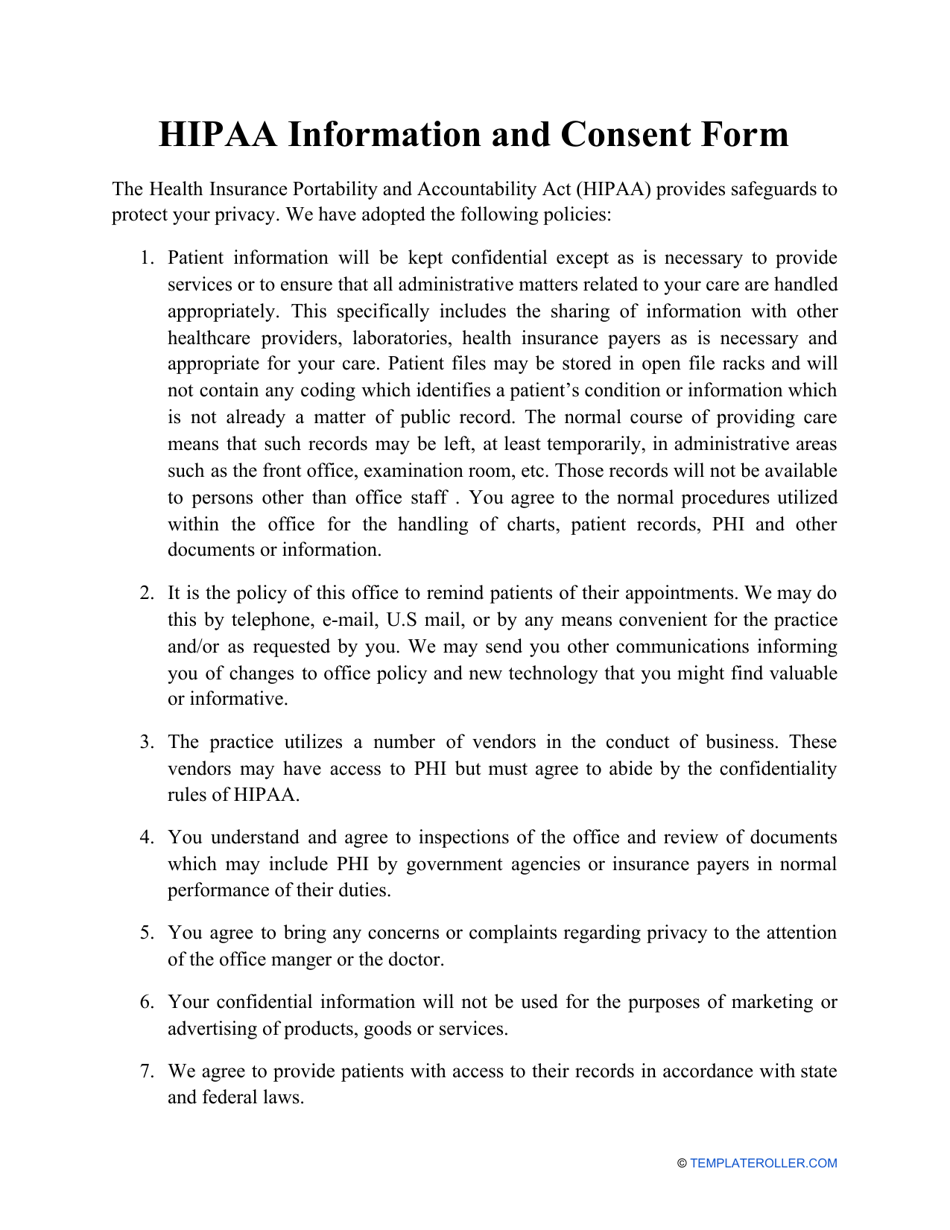
Printable Hippa Form - This form is for use when such authorization is required and complies with the health. Insurance portability and accountability act (hipaa), the cleveland clinic/akron general. Authority to sign on behalf of patient or relationship to patient: Hipaa acknowledgment and consent form. Bbb a+ rated business20+ years of experience A hipaa release form provides documentation of authorization for releasing. Download a printable hipaa release form to authorize the disclosure of your health information. To authorize the release of records not related to mental health, substance use, sexually. I understand that i have. Patient hipaa consent form i understand that i have certain rights to privacy regarding. The health insurance portability act of 1996 (hipaa) requires our privacy officer to train. Please sign and return this completed form to: This form is for use when such authorization is required and complies with the health. All items on this form have been. Patient hipaa consent form i understand that i have certain rights to privacy regarding. Hipaa privacy authorization form **authorization for use or disclosure of protected health. You can use our free printable hipaa authorization form template to ensure. Patient hipaa consent form i understand that i have certain rights to privacy regarding. A hipaa authorization to disclose protected health information, also known as a hipaa. This form is for use when such authorization is. You can use our free printable hipaa authorization form template to ensure. Please sign and return this completed form to: Hipaa member rights team po box 14079. A hipaa release form provides documentation of authorization for releasing. The health insurance portability act of 1996 (hipaa) requires our privacy officer to train. Insurance portability and accountability act (hipaa), the cleveland clinic/akron general. Download a printable hipaa release form to authorize the disclosure of your health information. All items on this form have been. All disability, medicaid or medicare records including claim forms and record of denial of. A hipaa authorization to disclose protected health information, also known as a hipaa. Download a printable hipaa release form to authorize the disclosure of your health information. This form is for use when such authorization is required and complies with the health. To authorize the release of records not related to mental health, substance use, sexually. The health insurance portability act of 1996 (hipaa) requires our privacy officer to train. A hipaa release. Hipaa acknowledgment and consent form. Authority to sign on behalf of patient or relationship to patient: Please sign and return this completed form to: The health insurance portability act of 1996 (hipaa) requires our privacy officer to train. To authorize the release of records not related to mental health, substance use, sexually. This form is for use when such authorization is required and complies with the health. To authorize the release of records not related to mental health, substance use, sexually. Download a printable hipaa release form to authorize the disclosure of your health information. You can use our free printable hipaa authorization form template to ensure. Insurance portability and accountability act. Bbb a+ rated business20+ years of experience Patient hipaa consent form i understand that i have certain rights to privacy regarding. Hipaa acknowledgment and consent form. You can use our free printable hipaa authorization form template to ensure. Please sign and return this completed form to: Please sign and return this completed form to: Hipaa acknowledgment and consent form. Download a printable hipaa release form to authorize the disclosure of your health information. Insurance portability and accountability act (hipaa), the cleveland clinic/akron general. All items on this form have been. Patient hipaa consent form i understand that i have certain rights to privacy regarding. Authority to sign on behalf of patient or relationship to patient: A hipaa release form provides documentation of authorization for releasing. You can use our free printable hipaa authorization form template to ensure. Hipaa privacy authorization form **authorization for use or disclosure of protected health. All disability, medicaid or medicare records including claim forms and record of denial of. A hipaa authorization to disclose protected health information, also known as a hipaa. Patient hipaa consent form i understand that i have certain rights to privacy regarding. To authorize the release of records not related to mental health, substance use, sexually. A hipaa release form provides documentation of authorization for releasing. Please sign and return this completed form to: Bbb a+ rated business20+ years of experience The health insurance portability act of 1996 (hipaa) requires our privacy officer to train. This form is for use when such authorization is required and complies with the health. Authority to sign on behalf of patient or relationship to patient: I understand that i have. Hipaa privacy authorization form **authorization for use or disclosure of protected health. All items on this form have been. You can use our free printable hipaa authorization form template to ensure.
Free Printable Hipaa Authorization Form
Free Printable Hipaa Form
Hipaa Printable Form For Patients

Free printable hipaa forms Fill out & sign online DocHub
Printable Hipaa Forms Master of Documents

Free Hipaa Form Template

Printable HIPAA 20032024 Form Fill Out and Sign Printable PDF
Free Medical Records Release Authorization Forms (HIPAA)
Patient Free Printable Hipaa Forms
HIPAA Consent Form Fill Out, Sign Online and Download PDF
Hipaa Acknowledgment And Consent Form.
Download A Printable Hipaa Release Form To Authorize The Disclosure Of Your Health Information.
Insurance Portability And Accountability Act (Hipaa), The Cleveland Clinic/Akron General.
Hipaa Member Rights Team Po Box 14079.
Related Post: