Cms Form 1500 Printable
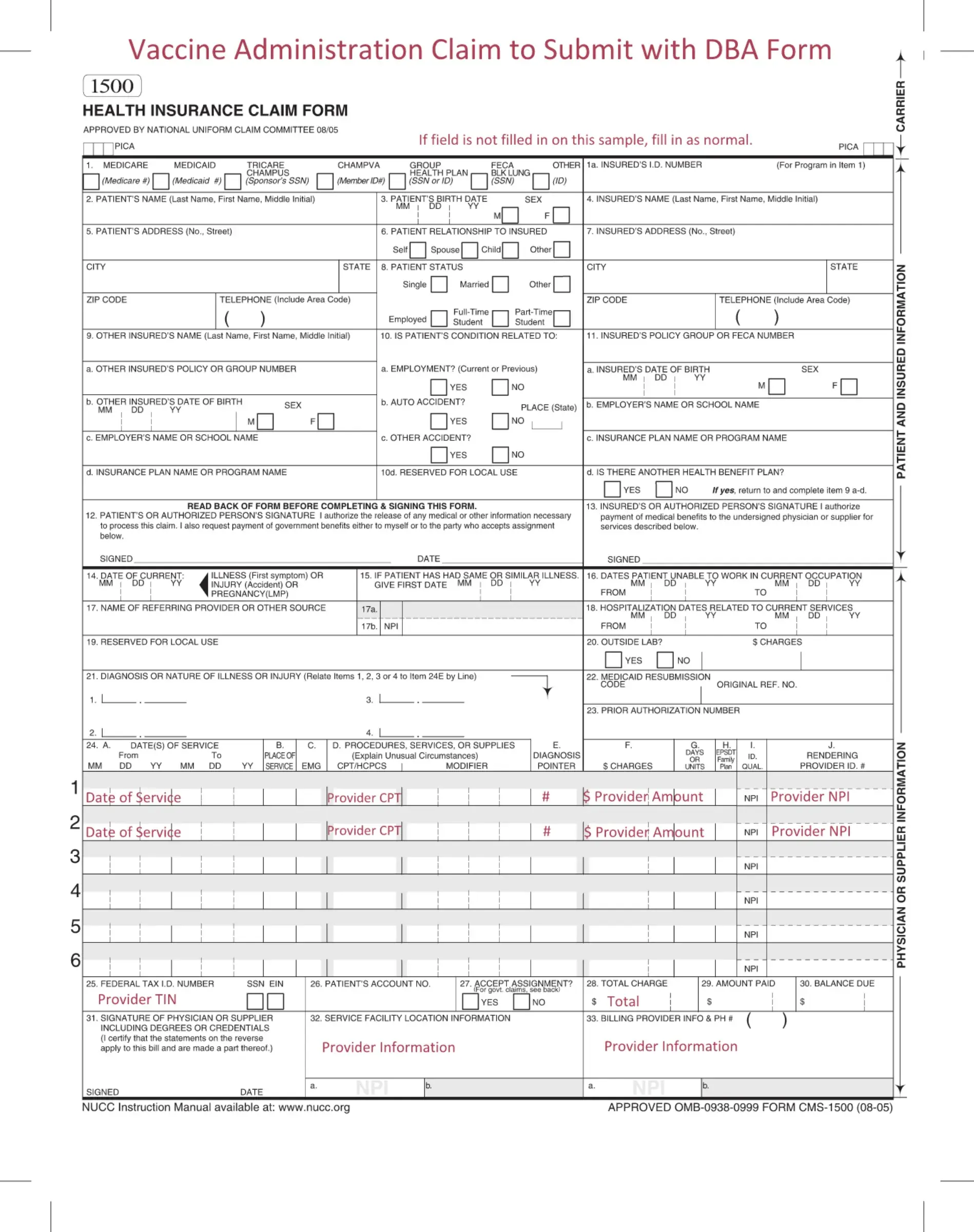
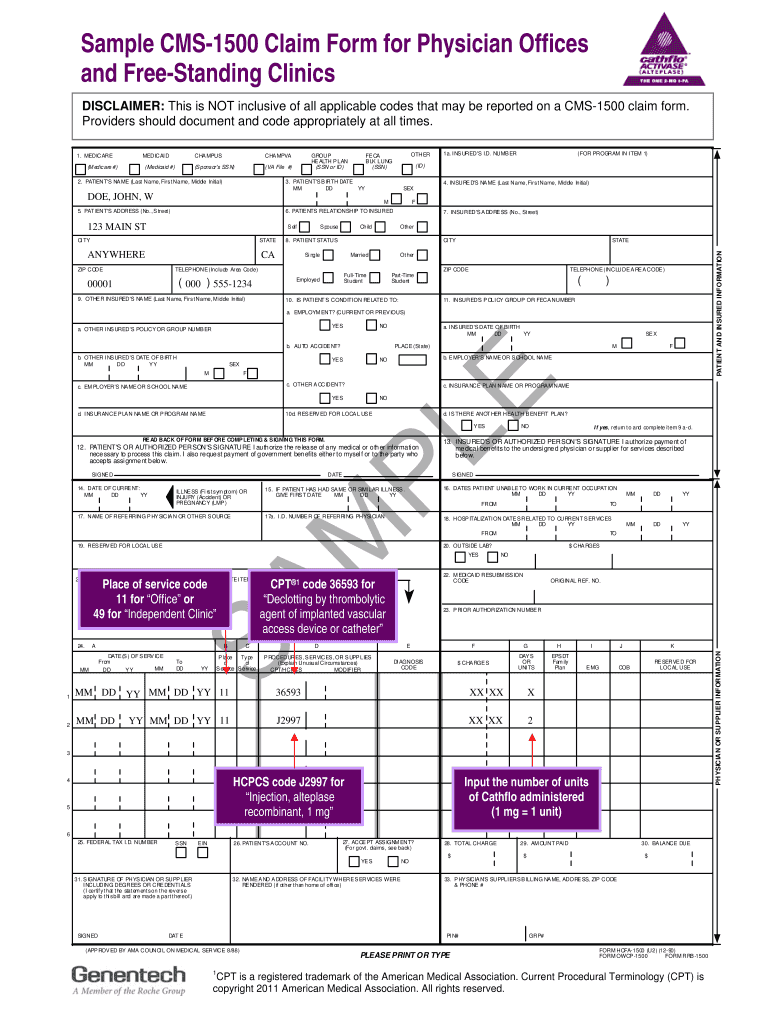
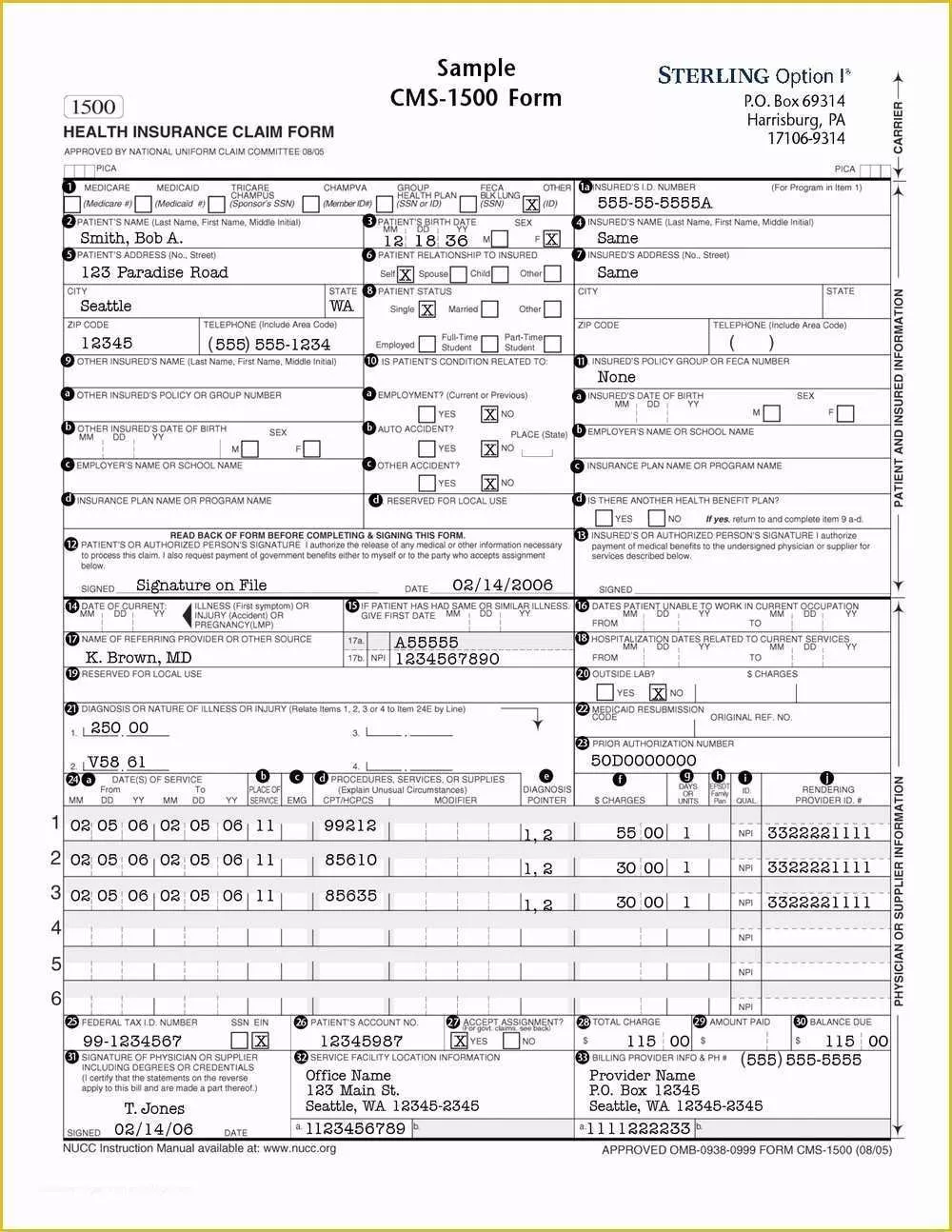
Cms Form 1500 Printable - The carrier section, the patient and insured information, and the physician and supplier information. Download free cms 1500 claim form fillable template. Download the blank form in pdf and word formats. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b. We'll focus on specific items with. Download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. Insured's or authorized person's signature i authorize payment of medical benefits to the. We are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs. The current version of the original manual from the national uniform claim. Save time with easy filling and printing. We'll focus on specific items with. In addition to medicare parts a/b and for medicare durable medical equipment. The carrier section, the patient and insured information, and the physician and supplier information. Download the blank form in pdf and word formats. We are authorized by cms, champus and owcp to ask you for information needed in the administration of the. We are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs. In addition to medicare parts a/b and for medicare durable medical equipment. Read the instructions and tips below first. Download the blank form in pdf and word formats. Claims may be electronically submitted to. We are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b. Read the instructions and tips below first. Download the blank form in pdf and word formats.. The current version of the original manual from the national uniform claim. We'll focus on specific items with. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b. Read the instructions and tips below first. Download the blank form in pdf and word formats. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b. We are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs. Download cms claim form 1500 which is used by health care professionals to bill medicare and. Download free cms 1500 claim form fillable template. The carrier section, the patient and insured information, and the physician and supplier information. The current version of the original manual from the national uniform claim. We are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs.. We'll focus on specific items with. Download free cms 1500 claim form fillable template. Read the instructions and tips below first. In addition to medicare parts a/b and for medicare durable medical equipment. We are authorized by cms, champus and owcp to ask you for information needed in the administration of the medicare, champus, feca, and black lung programs. Download free cms 1500 claim form fillable template. The carrier section, the patient and insured information, and the physician and supplier information. Save time with easy filling and printing. Insured's or authorized person's signature i authorize payment of medical benefits to the. Read the instructions and tips below first. Insured's or authorized person's signature i authorize payment of medical benefits to the. Download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. We'll focus on specific items with. In addition to medicare parts a/b and for medicare durable medical equipment. Download free cms 1500 claim form fillable template. Download the blank form in pdf and word formats. In addition to medicare parts a/b and for medicare durable medical equipment. We'll focus on specific items with. The carrier section, the patient and insured information, and the physician and supplier information. The current version of the original manual from the national uniform claim. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b. Read the instructions and tips below first. Download cms claim form 1500 which is used by health care professionals to bill medicare and medicaid. Download free cms 1500 claim form fillable template. Save time with easy filling and printing. The current version of the original manual from the national uniform claim. In addition to medicare parts a/b and for medicare durable medical equipment. Download the blank form in pdf and word formats. The carrier section, the patient and insured information, and the physician and supplier information.
Cms 1500 Printable Form

Cms 1500 Form Printable
Cms 1500 Claim Form Printable
Form Cms 1500 ≡ Fill Out Printable PDF Forms Online
Pdf Printable Cms 1500 Claim Form Printable Form 2024
Cms 1500 Printable Form
Cms 1500 Fillable Pdf Fill Online, Printable, Fillable, Blank pdfFiller
The Revised CMS1500 Claim Form Everything You Need to Know — Viscardi
Fillable Pdf Cms 1500 Form Printable Forms Free Online
Cms 1500 Claim Form Fillable Free Printable Forms Free Online
We'll Focus On Specific Items With.
We Are Authorized By Cms, Champus And Owcp To Ask You For Information Needed In The Administration Of The Medicare, Champus, Feca, And Black Lung Programs.
Insured's Or Authorized Person's Signature I Authorize Payment Of Medical Benefits To The.
Related Post: